A couple weeks ago I blogged hard about a problem presented by lesion studies of the anterior cingulate cortex (ACC), a broad swath of cortex shown to be involved in aspects of cognitive control such as conflict monitoring (Botvinick et al, 2001) and predicting error likelihood (Brown & Braver, 2005). Put simply: The annihilation of this region, either through strokes, infarctions, bullet wounds, or other cerebral insults, does not result in a deficit of cognitive control, as measured through reaction time (RT) in response to a variety of tasks, such as Stroop tasks - a task that requires overriding prepotent responses to a word presented on a screen, as opposed to the color of the ink that the word is written in - and paradigms which involve task-switching.
In particular, a lesion study by Fellows & Farah (2005) did not find a significant RT interaction of group (either controls or lesion patients) by condition (either low or high conflict in a Stroop task; i.e., either the word and ink color matched or did not match), suggesting that the performance of the lesion patients was essentially the same as the performance of controls. This in turn prompted the question of whether the ACC was really necessary for cognitive control, since those without it seemed to do just fine, and were about a pound lighter to boot. (Rimshot)
However, a recent study by Sheth et al (2012) in Nature examined six lesion patients undergoing cingulotomy, a surgical procedure which removes a localized portion of the dorsal anterior cingulate (dACC) in order to alleviate severe obsessive-compulsive symptoms, such as the desire to compulsively check the amount of hits your blog gets every hour. Before the cingulotomy, the patients performed a multisource interference task designed to elicit cognitive control mechanisms associated with dACC activation. The resulting cingulotomy overlapped with the peak dACC activation observed in response to high-conflict as contrasted with low-conflict trials (Figure 1).
Furthermore, the pattern of RTs before surgery followed a typical response pattern replicated over several studies using this task: RTs were faster for trials immediately following trials of a similar type - such as congruent trials following congruent trials, or incongruent trials following incongruent trials - and RTs were slower for trials which immediately followed trials of a different type, a pattern known as the Gratton effect.
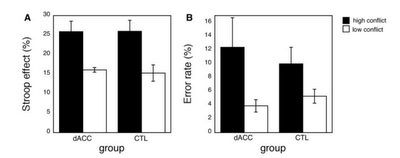
The authors found that global error rates and RTs were similar before and after the surgery, dovetailing with the results reported by Fellows & Farah (2005); however, the modulation of RT based on previous trial congruency or incongruency was abolished. These results suggest that the ACC functions as a continuous updating mechanism modulating responses based on the weighted past and on trial-by-trial cognitive demands, which fits into the framework posited by Dosenbach (2007, 2008) that outlines the ACC as part of a rapid-updating cingulo-opercular network necessary for quick and flexible changes in performance based on task demands and performance history.
Above all, this experiment illustrates how lesion studies ought to be conducted. First, the authors identified a small population of subjects about to undergo a localized surgical procedure to lesion a specific area of the brain known to be involved in cognitive control; the same subjects were tested before the surgery using fMRI and during surgery using single-cell recordings; and interactions were tested which had been overlooked by previous lesion studies. It is an elegant and simple design; although I imagine that testing subjects while they had their skulls split open and electrodes jammed into their brains was disgusting. The things that these sickos will do for high-profile papers.
(This study may be profitably read in conjunction with a recent meta-analysis of lesion subjects (Gläscher et al, 2012; PNAS) dissociating cortical structures involved in cognitive control as opposed to decision-making and evaluation tasks. I recommend giving both of these studies a read.)
In particular, a lesion study by Fellows & Farah (2005) did not find a significant RT interaction of group (either controls or lesion patients) by condition (either low or high conflict in a Stroop task; i.e., either the word and ink color matched or did not match), suggesting that the performance of the lesion patients was essentially the same as the performance of controls. This in turn prompted the question of whether the ACC was really necessary for cognitive control, since those without it seemed to do just fine, and were about a pound lighter to boot. (Rimshot)
However, a recent study by Sheth et al (2012) in Nature examined six lesion patients undergoing cingulotomy, a surgical procedure which removes a localized portion of the dorsal anterior cingulate (dACC) in order to alleviate severe obsessive-compulsive symptoms, such as the desire to compulsively check the amount of hits your blog gets every hour. Before the cingulotomy, the patients performed a multisource interference task designed to elicit cognitive control mechanisms associated with dACC activation. The resulting cingulotomy overlapped with the peak dACC activation observed in response to high-conflict as contrasted with low-conflict trials (Figure 1).
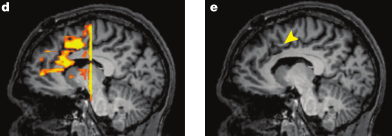 |
| Figure 1 reproduced from Sheth et al (2012). d) dACC activation in response to conflict. e) arrow pointing to lesion site |
Furthermore, the pattern of RTs before surgery followed a typical response pattern replicated over several studies using this task: RTs were faster for trials immediately following trials of a similar type - such as congruent trials following congruent trials, or incongruent trials following incongruent trials - and RTs were slower for trials which immediately followed trials of a different type, a pattern known as the Gratton effect.
The authors found that global error rates and RTs were similar before and after the surgery, dovetailing with the results reported by Fellows & Farah (2005); however, the modulation of RT based on previous trial congruency or incongruency was abolished. These results suggest that the ACC functions as a continuous updating mechanism modulating responses based on the weighted past and on trial-by-trial cognitive demands, which fits into the framework posited by Dosenbach (2007, 2008) that outlines the ACC as part of a rapid-updating cingulo-opercular network necessary for quick and flexible changes in performance based on task demands and performance history.
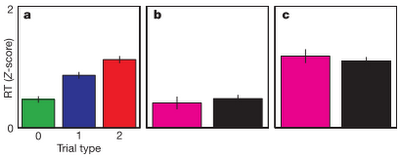 |
| a) Pre-surgical RTs in response to trials of increasing conflict. b, c) Post-surgical RTs showing no difference between low-conflict trials preceded by either similar or different trial types (b), and no RT difference between high-conflict trials preceded by either similar or different trial types (c). |
Above all, this experiment illustrates how lesion studies ought to be conducted. First, the authors identified a small population of subjects about to undergo a localized surgical procedure to lesion a specific area of the brain known to be involved in cognitive control; the same subjects were tested before the surgery using fMRI and during surgery using single-cell recordings; and interactions were tested which had been overlooked by previous lesion studies. It is an elegant and simple design; although I imagine that testing subjects while they had their skulls split open and electrodes jammed into their brains was disgusting. The things that these sickos will do for high-profile papers.
(This study may be profitably read in conjunction with a recent meta-analysis of lesion subjects (Gläscher et al, 2012; PNAS) dissociating cortical structures involved in cognitive control as opposed to decision-making and evaluation tasks. I recommend giving both of these studies a read.)