
(Note: I recently completed my candidacy exam, which involved writing a trio of papers focusing on different aspects of my research. Most of this post is cannibalized from a section I wrote on lesion studies of the anterior cingulate cortex, which produce counterintuitive results when contrasted to lesions of other areas, such as the DLPFC and OFC, which do indeed seem to disrupt the processes that those regions are implicated in from the neuroimaging literature.
My work primarily involves healthy people with intact brains, and observing indirect measures of neural firing through tracking slow blood flow changes in the brain. However, "activation" as defined by fMRI is not the same as the underlying neural dynamics, and, barring invasive single-cell recordings, we have few options for directly measuring neural firing in response to different tasks and psychological contexts. This caveat inherent in fMRI research becomes particularly important when interpreting the results of lesion studies.)
Although the majority of the neuroimaging literature has implicated the dACC as playing a critical role in the signaling for cognitive control when necessary, the most direct test of a brain structure’s necessity in a cognitive process is through examining subjects presenting with lesions in that part of the brain. For example, if it can be demonstrated that a subject without an ACC still performs equivalent to controls on tasks involving cognitive control, then that would argue against the necessity of that area’s involvement in the hypothesized cognitive process. Studies involving human subjects with lesions are relatively rare and suffer from low power, but can still reveal important aspects of neural functioning.
Bottom line: If the inferences from neuroimaging studies are to believed, then the ACC is necessary somehow for cognitive control or executive function; however, lesion studies belie this claim, suggesting perhaps that the necessary processes for these cognitive functions take place elsewhere and merely light up the ACC as some sort of epiphenomenon. Admittedly, I am unsure of what to make of all this. The most useful experiments to carry out, in my opinion, would be to apply transcranial magnetic stimulation (TMS) to temporarily knock out this area in healthy controls, and then observe what happens; however, as TMS is only able to disrupt neural firing on surface areas of the cortex, stimulation of deeper areas remains impractical. With continuing advances in the ability of TMS to stimulate deeper cortical (and, possibly, subcortical?) structures, we may get a better grasp of what is going on.
My work primarily involves healthy people with intact brains, and observing indirect measures of neural firing through tracking slow blood flow changes in the brain. However, "activation" as defined by fMRI is not the same as the underlying neural dynamics, and, barring invasive single-cell recordings, we have few options for directly measuring neural firing in response to different tasks and psychological contexts. This caveat inherent in fMRI research becomes particularly important when interpreting the results of lesion studies.)
Although the majority of the neuroimaging literature has implicated the dACC as playing a critical role in the signaling for cognitive control when necessary, the most direct test of a brain structure’s necessity in a cognitive process is through examining subjects presenting with lesions in that part of the brain. For example, if it can be demonstrated that a subject without an ACC still performs equivalent to controls on tasks involving cognitive control, then that would argue against the necessity of that area’s involvement in the hypothesized cognitive process. Studies involving human subjects with lesions are relatively rare and suffer from low power, but can still reveal important aspects of neural functioning.
The ACC, in particular, has been the subject of several
lesion studies that have shown conflicting and counterintuitive results. For
example, a single-subject lesion study of a patient with left ACC damage
exhibited both smaller ERNs and increased RT in response to incongruent stimuli
in a spatial Stroop paradigm. This study showed that conflict monitoring and
error detection, at least in this patient, do not both come from the same area
of ACC, suggesting that these processes occur in different areas. However, while
the ERN was shown to be attenuated in the patient, the conflict response (a
waveform called the N450) was actually enhanced (Swick & Turken, 2002). This suggests that conflict monitoring occurs in a nearby
prefrontal area, such as the DLPFC, before information about the conflict is
sent to the ACC.
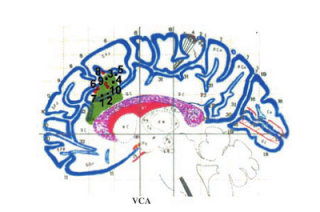 |
| Figure of the lesion for the single subject analyzed by Turken & Swick (2002). Overlaid are coordinates of peak activation for conflict-related tasks from other studies. |
On the other hand, a lesion
study conducted by Fellows
& Farah (2005) compared the performance of individuals with dACC lesions to
that of controls across a battery of tasks hypothesized to involve cognitive
control. These tasks included a Stroop task and a go-nogo task which are known
to elicit significantly greater increases in RT after errors, and to induce
significantly greater amounts of errors during incongruent trials. The results
showed no significant interactions between group and task, suggesting that the
dACC is not necessary for the implementation of cognitive control. Furthermore,
the authors pointed out that tasks involving cognitive control may be
confounded with emotional responding, which in turn could simply be associated
with the ACC's involvement in regulating muscle tone. In any case, it is apparent
that although this structure is somehow associated with cognitive control, it
is not strictly necessary for it.
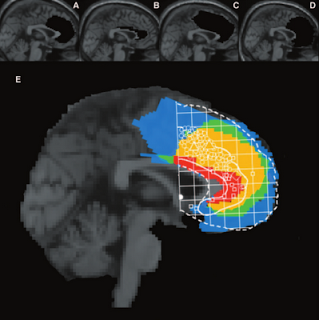 |
| Figure showing group overlap of lesions in the Fellows & Farah (2005) study. Circles and squares represent an overlay of a meta-analysis by Bush et al (2000), with circles representing peak activations for cognitive tasks, and squares representing peak activations for emotional tasks. |
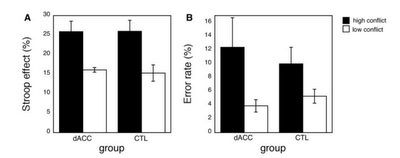 |
| Comparison of Stroop effect (measured in percent signal change from mean congruent trial RT) and error rate between lesion patients and controls. No significant difference was found on either measure between the two groups. |
In
sum, these lesion studies suggest that the dACC may not be indispensable for
signaling the DLPFC to implement cognitive control. However an alternative explanation
is that patients with ACC lesions are usually ipsilateral, and that furthermore
they may be compensating for required cognitive control by recruiting nearby
cortical areas. However, two lines of evidence argue against this
interpretation. First, one of the lesion patients examined in the Fellows &
Farah (2005) had extensive medial ACC damage encompassing
dACC bilaterally, but showed a similar pattern of error rates and RT difference
between congruent and incongruent conditions as did the other lesion patients
and the control group. Secondly, lesion studies of other areas of the brain –
such as the orbitofrontal cortex – have shown that those regions appear to be
specific to the cognitive processes they are hypothesized to be involved in.
For example, patients with OFC lesions exhibit significantly impaired
performance in decision-making tasks such as the Iowa Gambling Task and
Wisconsin Card Sorting Task, as well as decreased autonomic activity in
response to highly risky gambles (Bechara et al,
1994). Even though the patients in this study had
suffered from their lesions for a comparable amount of time as the lesion
subjects in the Fellows & Farah (2005) study, there was no evidence of
recruitment of other cortical areas in order to support their deficits in
decision-making.
However, although these lesion studies
have shown no significant differences in error rates between the lesion
patients and controls, other experiments have revealed that patients with ACC
damage are less likely to correct for their mistakes on trials immediately
following an error. In addition, patients with ACC lesions are less likely to
be aware that an error has occurred (Swick & Turken, 2002). These results
suggest that there may be a necessary role for of the ACC for the actual
detection of errors, which would be consistent with the hypothesis that this
area is involved in the comparison of actions against their predicted outcomes.
How lesions affect the transfer of information from the ACC to the DLPFC and
other cortical regions supposedly involved in the implementation of cognitive control,
however, is less well understood.
Bottom line: If the inferences from neuroimaging studies are to believed, then the ACC is necessary somehow for cognitive control or executive function; however, lesion studies belie this claim, suggesting perhaps that the necessary processes for these cognitive functions take place elsewhere and merely light up the ACC as some sort of epiphenomenon. Admittedly, I am unsure of what to make of all this. The most useful experiments to carry out, in my opinion, would be to apply transcranial magnetic stimulation (TMS) to temporarily knock out this area in healthy controls, and then observe what happens; however, as TMS is only able to disrupt neural firing on surface areas of the cortex, stimulation of deeper areas remains impractical. With continuing advances in the ability of TMS to stimulate deeper cortical (and, possibly, subcortical?) structures, we may get a better grasp of what is going on.